ICRA Class IV vs. Class V: A Bay Area Hospital Containment Guide
Bay Area hospitals, medical centers, and ambulatory surgery centers are in a near-continuous state of renovation. Seismic retrofits, infrastructure modernization, and expanding clinical capacity mean construction activity coexists with some of the most vulnerable patient populations in the country. When that activity crosses into high-risk or highest-risk clinical zones, two ICRA classifications define the containment stakes: Class IV and Class V.
Getting the distinction right is not a formality. It is the difference between an acceptable dust barrier and a life-safety system that protects immunocompromised patients from potentially fatal airborne pathogens. This guide breaks down the core differences between the two classifications, explains what California and Bay Area regulations layer on top of the national ICRA framework, and outlines how professional containment contractors keep complex hospital projects on the right side of compliance.
What the ICRA 2.0 Matrix Actually Requires
The Infection Control Risk Assessment (ICRA) framework, maintained by the American Society for Healthcare Engineering (ASHE), uses a risk matrix that intersects two variables: Construction Activity Type (A through D) and Patient Risk Group (Low, Medium, High, and Highest). The ASHE ICRA 2.0 Tool and Permit is the definitive document facilities managers and general contractors must reference when scoping containment on any licensed healthcare project.
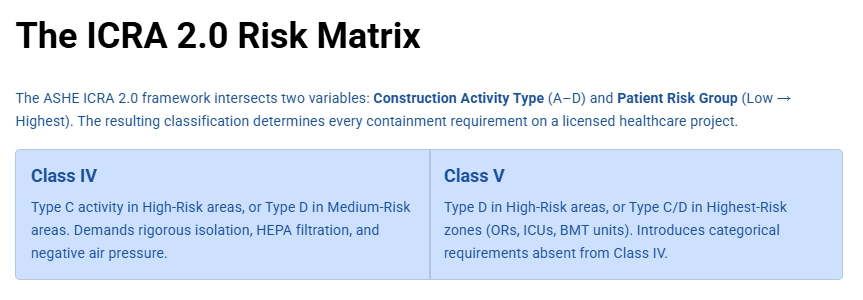
Class IV: High-Risk Activity in High-Risk Areas
Class IV is triggered when Type C activities (moderate to high dust generation, such as cutting drywall or coring concrete) occur in High-Risk patient areas, or when Type D activities (major demolition and construction) take place in Medium-Risk areas. State health agencies summarize this threshold clearly: Class IV represents significant potential exposure and demands rigorous physical isolation, HEPA filtration, and negative air pressure.
Class V: The Highest-Risk Standard
Class V was introduced in the ICRA 2.0 update specifically to address extreme clinical risk environments. It activates when Type D activities occur in High-Risk areas, or when Type C or D activities reach Highest-Risk zones such as operating rooms, bone marrow transplant units, and ICUs. Healthcare construction compliance resources note that Class V is not simply a stricter version of Class IV. It introduces categorical requirements that do not appear at lower classifications at all.
The Engineering Differences Between Class IV and Class V
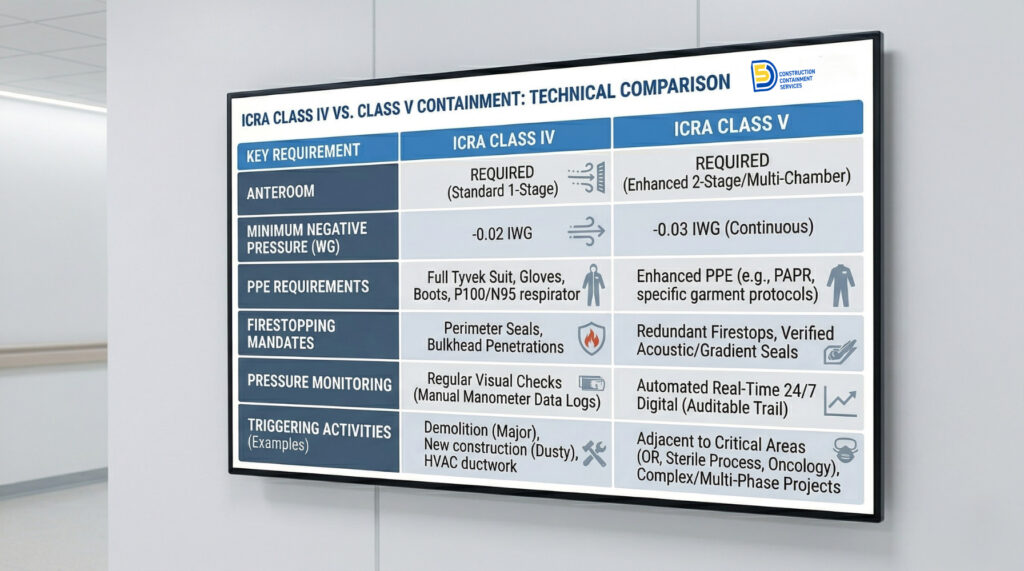
Both Class IV and Class V require physical isolation, negative air pressure relative to the surrounding clean corridor, and exhaust through 99.97% HEPA filtration. The differences lie in what Class V mandates that Class IV does not.
Anteroom Requirements
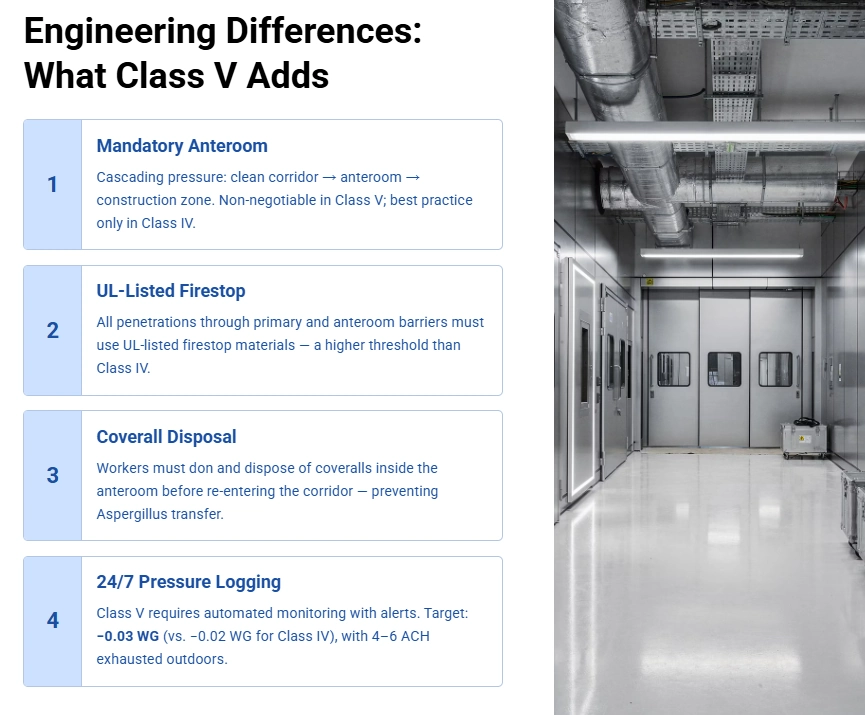
Class V requires a mandatory anteroom large enough to stage equipment and allow full worker decontamination before re-entering the clean corridor. The anteroom itself must maintain a cascading pressure relationship: air flows from the clean hospital corridor into the anteroom, and from the anteroom into the construction zone, never in reverse. Infection control and construction resources emphasize that this cascading design is non-negotiable in Class V environments. Class IV projects often use an anteroom as a best practice, but Class V makes it an absolute requirement.
Firestop and Penetration Sealing
Class V strictly requires that all penetrations through both the primary barrier and anteroom barriers be sealed with UL-listed firestop materials. Every conduit, pipe sleeve, and cable run through the barrier must be documented and treated. Class IV requires penetration sealing as well, but the Class V specification demands the UL listing, which is a higher threshold than simply applying any approved sealant.
Personnel Protective Equipment
In Class V environments, workers must wear disposable coveralls at all times while inside the containment zone. Before re-entering the hospital corridor, they must remove and dispose of those coveralls inside the anteroom. This requirement is designed to prevent fungal spores, particularly Aspergillus species, from being carried on clothing into areas where immunocompromised patients are present. Class IV requires rigorous PPE protocols but does not impose the same mandatory coverall disposal procedure.
Continuous Negative Air Monitoring
Both Class IV and V require continuous monitoring with a recording manometer, but Class V elevates this to 24/7 automated logging with alert systems. The standard negative pressure target for Class IV is a minimum of -0.02 inches of water gauge (WG), while Class V typically requires -0.03 WG or higher in Highest-Risk zones. The system must deliver a minimum of 4 to 6 Air Changes per Hour (ACH), with exhaust discharged directly to the outdoors through HEPA filters and not recirculated.
Why Barrier Material Choice Is a Compliance Decision
The physical containment wall itself is often where ICRA compliance succeeds or fails in practice. Three primary barrier approaches circulate in the industry, and only one consistently meets Class IV and V requirements without compromise.
Plastic Sheeting
Plastic poly sheeting is inadequate for Class IV or V containment. It tears under typical construction activity, provides negligible sound attenuation, and “bellows” under negative air pressure, physically destroying the airtight seal the classification requires. Industry analysis on containment barrier materials makes clear that poly is appropriate for lower-risk classifications only. Using it in a Class IV or V environment is not a cost-saving measure; it is a compliance failure.
Traditional Drywall
Drywall offers rigidity, but installation and demolition generate significant quantities of respirable gypsum and crystalline silica dust. These are the very contaminants ICRA containment is designed to prevent. Modular construction resources document this contradiction clearly. Drywall is also time-intensive to install and remove, and generates construction debris that must be managed as a separate waste stream inside the containment zone.
Modular Temporary Wall Systems
Rigid modular temporary wall systems represent the industry benchmark for Class IV and V environments. These systems use composite panels with integrated gaskets that create a mechanical, airtight seal against floors and ceilings without tape, adhesive, or dust generation. Healthcare containment research consistently identifies modular systems as the superior solution for occupied healthcare facilities. The key advantages include faster installation with no dust, reusability across projects, and documented compliance performance with ICRA Class IV and V specifications.
At 5DCCS, our full-service modular containment installations use systems specifically engineered for high-acuity clinical environments. Learn more about the standards these systems meet on our
ICRA-compliant containment walls page
What Goes Wrong When Classification Is Ignored
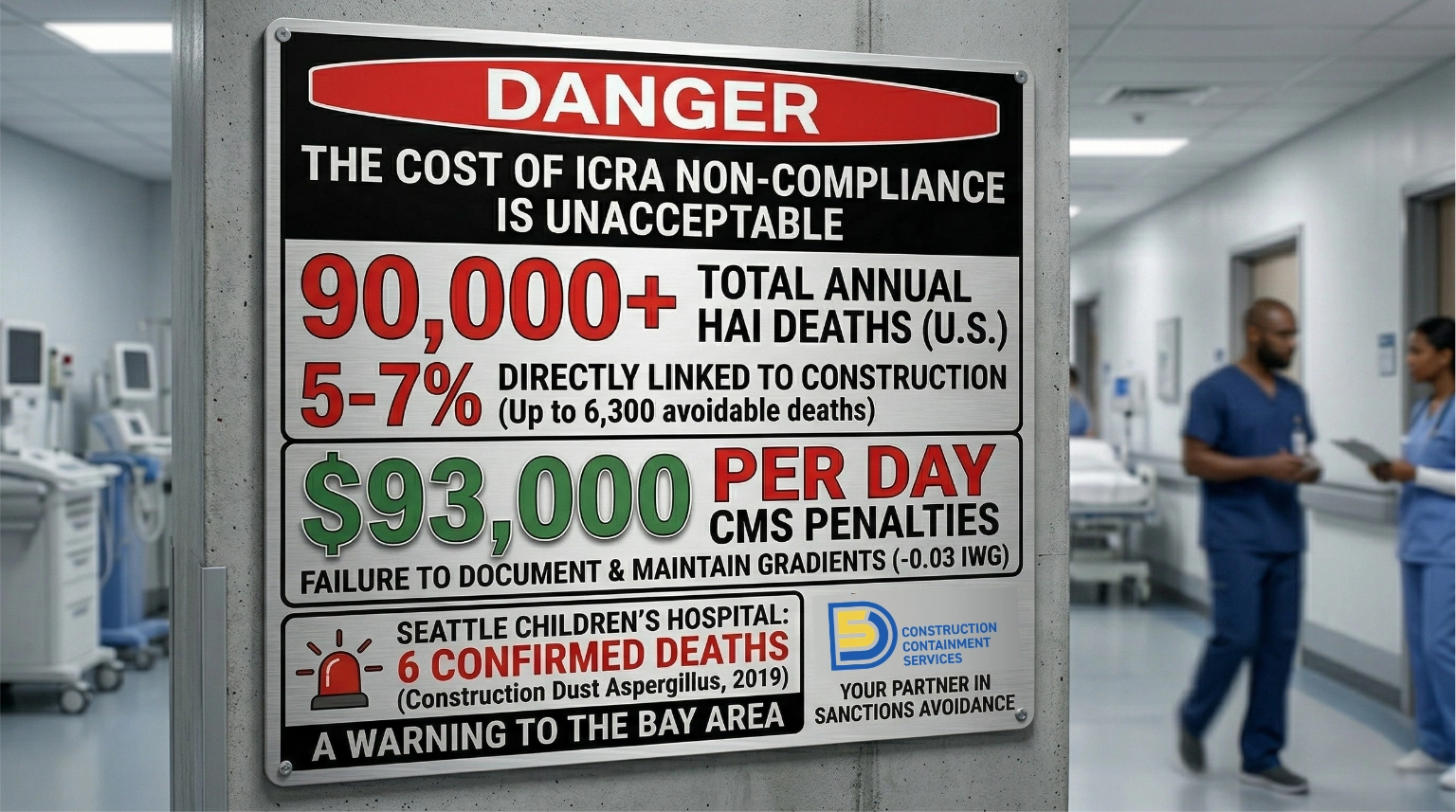
The public health consequences of improper ICRA containment in hospital environments are not theoretical. Conservative estimates attribute 5 to 7 percent of the roughly 90,000 annual healthcare-associated infection (HAI) deaths in the United States to construction-related activities. Legal and regulatory analysis of HAI liability documents the growing scrutiny that infection preventionists and legal counsel are placing on construction-period infection events.
The most frequently implicated pathogen in construction-related HAIs is Aspergillus fumigatus, a mold species whose spores become airborne when soil and building materials are disturbed. For patients with compromised immune systems, including transplant recipients, oncology patients, and premature infants, even a brief exposure can be lethal.
The outbreak record at Seattle Children’s Hospital illustrates the severity: an Aspergillus outbreak linked to HVAC system contamination infected 14 patients and caused 6 deaths between 2001-2019. Investigative reporting on that case highlights how persistent mold contamination in a healthcare facility can evade detection for years when systemic controls are not maintained.
Regulatory and Financial Consequences
The Joint Commission and the Centers for Medicare and Medicaid Services (CMS) enforce physical environment standards during surveys. Condition-level deficiencies in the physical environment category can result in civil monetary penalties reaching $93,000 per day. Healthcare construction best practices resources note that these penalties compound daily until the deficiency is corrected and verified, making proper initial containment far less costly than the remediation alternative.
There is also an indirect financial consequence tied to patient experience. Poor HCAHPS scores resulting from construction noise directly reduce a hospital’s Medicare reimbursement under the Value-Based Purchasing program. Research on noise and HCAHPS scoring documents the correlation between construction-period noise complaints and reduced patient satisfaction scores. Modular containment systems substantially outperform poly sheeting and drywall on acoustic attenuation, providing a practical path to protecting both patients and reimbursement rates.
The Bay Area and California Regulatory Layer
California healthcare construction operates under a regulatory framework that exceeds the baseline national ICRA standards in several important respects.
HCAI Plan Review and the Inspector of Record
The Healthcare Infrastructure Division of the California Department of Health Care Access and Information (HCAI), formerly known as OSHPD, has jurisdiction over construction in all licensed healthcare facilities in the state. Every project in a licensed California hospital or skilled nursing facility requires HCAI plan review and an approved Inspector of Record (IOR) physically present on site. The IOR is responsible for verifying that construction activity, including containment installation and maintenance, complies with approved plans at every phase.
California also imposes rigorous Cal/OSHA enforcement through its crystalline silica standard, which governs respirable silica generated during construction activities. Any cutting, grinding, or demolition of concrete, masonry, or similar materials in a Bay Area hospital project must comply with these exposure limits. This reinforces why dust-generating barrier materials like drywall are counterproductive in Class IV and V environments.
The California Department of Public Health (CDPH) similarly requires vigilant infection prevention during all construction and maintenance in licensed facilities, including during routine maintenance that may generate dust or disrupt concealed building systems.
The Scale of Bay Area Healthcare Construction
Bay Area health systems are currently executing large-scale, highly regulated infrastructure programs. The San Francisco VA Medical Center, for example, is midway through a $57M seismic retrofit and comprehensive renovation program managed in coordination with the U.S. Army Corps of Engineers. Project details from the VA illustrate the complexity of managing active clinical operations alongside major structural work. That is exactly the environment where Class IV and V containment protocols are essential.
Projects of this scale require containment contractors who understand not only the ICRA matrix but also the HCAI inspection process, IOR coordination protocols, and the specific phasing requirements that keep active patient care areas fully separated from construction zones throughout a multi-year project.
How 5DCCS Approaches Class IV and Class V Projects in the Bay Area
Based in San Jose, 5DCCS is a Northern California specialist focused exclusively on professional containment services for occupied healthcare, education, and government facilities. Our full-service model is particularly well-suited to Class IV and V hospital environments, where the speed of installation, quality of seal, and zero dust generation during setup all directly affect patient safety.
Here is what full-service containment means in practice on a Class IV or V hospital project:
- Pre-construction ICRA documentation review: 5DCCS reviews the project’s ICRA permit and risk matrix before mobilization to confirm the correct classification, barrier specifications, and monitoring requirements.
- Modular wall system installation: Our team installs rigid modular panel systems that create a mechanical floor-to-deck seal without adhesives, tape, or dust. All penetrations are sealed with appropriate firestop materials per Class V requirements where applicable.
- Negative air setup and monitoring: We coordinate with the GC and facility’s infection preventionist to establish proper pressure differentials, ACH rates, and monitoring protocols, including automated logging for Class V environments.
- Anteroom configuration: For Class V projects, 5DCCS designs and installs the anteroom as part of the initial containment assembly, ensuring sufficient staging space and proper directional airflow.
- Ongoing maintenance and dismantlement: Full-service means we maintain the containment throughout the project and remove it cleanly at completion with no gypsum debris, no adhesive residue, and no secondary cleaning burden for the hospital.
For facilities teams evaluating how containment service levels compare, our full-service vs. self-service containment overview walks through the cost and operational tradeoffs in detail. For occupied public facilities, and especially for Class IV and V hospital environments, full-service consistently delivers faster installation, lower total project disruption, and cleaner compliance documentation.
Bay Area general contractors and hospital facilities managers can also explore our services page for a complete picture of containment solutions across project types and ICRA classifications.
Frequently Asked Questions About ICRA Class IV and Class V in Bay Area Hospitals
Getting ICRA Containment Right the First Time

The gap between ICRA Class IV and Class V is not a bureaucratic footnote. It reflects real differences in clinical risk, and the containment system must match that risk precisely. In Bay Area hospitals operating under HCAI jurisdiction, with Joint Commission and CMS surveys always on the horizon, the cost of getting it wrong is measured not just in dollars but in patient outcomes.
Professional, full-service containment from an experienced contractor is the most reliable path to Class IV and V compliance and to keeping construction timelines on track in facilities where every square foot of operational space carries clinical value.
5DCCS is ready to scope your next Bay Area hospital containment project. Contact us through our contact page to discuss project details, timeline, and the right containment approach for your ICRA classification.